Malignant
Cancer and Malignancy
 |
|
Cancer is a group of diseases characterized by uncontrolled cell division leading to growth of abnormal tissue. It is believed that cancers arise from both genetic and environmental factors that lead to aberrant growth regulation of a stem cell population, or by the dedifferentiation of more mature cell types.
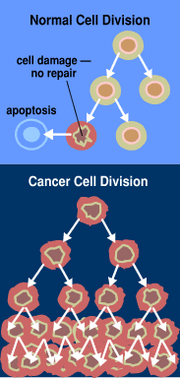
Cell multiplication (proliferation) is a normal physiologic process that occurs in almost all tissues and under many circumstances, such as response to injury, immune responses, or to replace cells that have died or have been shed as a part of their lifecycle (in tissues such as skin or the mucous membranes of the digestive tract). Normally the balance between proliferation and cell death is tightly regulated to ensure the integrity of organs and tissues. Mutations in DNA that lead to cancer appear to disrupt these orderly processes.
The uncontrolled and often rapid proliferation of cells can lead to either a benign tumor or a malignant tumor (cancer). Benign tumors do not spread to other parts of the body or invade other tissues, and they are rarely a threat to life. Malignant tumors can invade other organs, spread to distant locations (metastasize) and become life threatening.
Signs and symptoms
While advanced cancer may cause pain, it is not always the first symptom. Roughly, cancer symptoms can be divided into three groups:
- Local symptoms: unusual swelling (tumor in Latin means swelling), hemorrhage (bleeding), ulceration or jaundice.
- Symptoms of metastasis (spreading): enlarged lymph nodes, cough and hemoptysis, hepatomegaly (enlarged liver), bone pain, fracture of affected bones and neurological symptoms.
- Systemic symptoms: weight loss, poor appetite and cachexia, excessive sweating (night sweats), anemia, and specific paraneoplastic phenomena , i.e. specific conditions that are due to an active cancer, such as thrombosis or hormonal changes.
Every single item in the above list has a substantial differential diagnosis (it may be associated with unrelated diseases). Often, cancer is an unexpected finding during investigation for much more common symptoms, while others are diagnosed through screening (see below).
Types of cancer
Cancers originate within a single cell. Hence, cancers can be classified by the type of cell in which it originates and by the location of the cell.
Carcinomas originate in epithelial cells, e.g. skin, digestive tract or glands. Leukemia starts in the bone marrow stem cells. Lymphoma is a cancer originating in lymphatic tissue. Melanoma arises in melanocytes. Sarcoma begins in the connective tissue of bone or muscle. Teratoma begins within germ cells.
Adult cancers
Adult cancers usually form in epithelial tissues and are believed often to be the result of a long biological process related to the interaction of exogenous exposures with genetic and other endogenous characteristics among susceptible people. Examples include: bladder carcinoma, blood (and bone marrow) - hematological malignancies, leukemia, lymphoma, Hodgkin's disease, non-Hodgkin's lymphoma, multiple myeloma, brain tumor, breast cancer, cervical cancer, colorectal cancer - in the colon, rectum, anus, or appendix, esophageal cancer, endometrial cancer - in the uterus, hepatocellular carcinoma - in the liver, gastrointestinal stromal tumor (GIST), laryngeal cancer, lung cancer, mesothelioma - in the pleura or pericardium, oral cancer, osteosarcoma - in bones, ovarian cancer, pancreatic cancer, prostate cancer, renal cell carcinoma - in the kidneys, rhabdomyosarcoma - in muscles, skin cancer (including benign moles and dysplastic nevi), stomach cancer, testicular cancer, and thyroid cancer.
Childhood cancers
Cancer can also occur in young children, particularly infants. Here, the aberrant genetic processes that fail to safeguard against the clonal proliferation of cells with unregulated growth potential occur very early in life and progress very quickly.
The age of peak incidence of cancer in children occurs during the first year of life. Neuroblastoma is the most common infant malignancy, followed by the leukemias and the central nervous system cancers. Female infants and male infants have essentially the same overall cancer incidence rates, but white infants have substantially higher cancer rates than black infants for most cancer types. Relative survival for infants is very good for neuroblastoma, Wilms' tumor and retinoblastoma, but not for most other types of cancer. Childhood cancers include, from most frequently occurring to least: Neuroblastoma, leukemia, central nervous system, retinoblastoma, Wilms' tumor, germ cell, soft tissue sarcomas, hepatic, lymphomas, epithelial.
Diagnosing cancer
Biopsy
A biopsy leads to the definitive diagnosis of most malignancies. It requires the removal of cells and/or pieces of tissue for examination by a pathologist. The tissue diagnosis indicates the type of cell that is proliferating, its severity (degree of dysplasia), its extent and size, and - sometimes with help from cytogenetics and immunohistochemistry - prognostic and therapeutic determinants.
Biopsy can be curative if the whole lesion is removed; in this case, the borders of the sample are examined closely to see if all malignant tissue has truly been excised.
The nature of the biopsy depends on the organ that is sampled. Many biopsies (such as those of the skin, breast or liver) can happen on an outpatient basis. Biopsies of other organs are performed under anesthesia and require surgery.
Screening
Cancer screening is the widespread uses of tests to detect cancers in the population. It is often an inexpensive, noninvasive procedure. If signs of cancer are detected, more definitive and invasive followup tests are performed to confirm the diagnosis.
Screening for cancer can lead to earlier diagnosis. Early diagnosis may lead to extended life. A number of different screening tests have been developed. Colon cancer can be detected through fecal occult blood testing and colonoscopy, which reduces both colon cancer incidence and mortality, presumably through the detection and removal of precancerous polyps. Similarly, cervical cytology testing (using the Pap smear) leads to the identification and excision of precancerous lesions. Over time, such testing has been followed by a dramatic reduction of cervical cancer incidence and mortality. Breast cancers can be detected by breast self-examination and regular screening mammograms. Testicular self-examination – is recommended for men from the age of 15 years to detect testicular cancer. Prostate cancer can be screened for by a digital rectal exam along with annual prostate specific antigen blood testing.
Screening for cancer is controversial in cases when it is not yet known if this test actually saves lives. The controversy arises when it is not clear if the benefits of screening outweigh the risks of follow-up diagnostic tests and cancer treatments. For example: when screening for prostate cancer, the PSA test may detect small cancers that would never become life threatening, but once detected will lead to treatment. This situation, called overdiagnosis, puts men at risk for complications from unnecessary treatment such as surgery or radiation. Followup procedures used to diagnose prostate cancer (prostate biopsy) may cause side effects, including bleeding and infection. Prostate cancer treatment may cause incontinence (inability to control urine flow) and erectile dysfunction (erections inadequate for intercourse). For these reasons, it is important that the benefits and risks of diagnostic procedures and treatment be taken into account when considering whether to undertake cancer screening.
Use of medical imaging to search for cancer in people without clear symptoms is similarly marred with problems. There is a significant risk of detection of an incidentaloma - a benign lesion that may be interpreted as a malignancy and be subjected to potentially dangerous investigations.
Treatment of cancer
Cancer can be treated by surgery, chemotherapy, radiation therapy or other methods. The choice of therapy depends upon the location and grade of the tumor and the stage of the disease.
Surgery
If the tumor is localized, surgery is often the preferred treatment. Example procedures include prostatectomy for prostate cancer and mastectomy for breast cancer. The goal of the surgery can be either the removal of only the tumor, or the entire organ. Since a single cancer cell can grow into a sizeable tumor, removing only the tumor leads to a greater chance of recurrence. A margin of healthy tissue is often resected to allow for small amounts of residual tumor cells.
In addition to removal of the primary tumor, surgery is often necessary for staging, e.g. determining the extent of the disease and whether there has been metastasis to regional lymph nodes. Staging determines the prognosis and the need for adjuvant therapy.
Chemotherapy
Chemotherapy is the treatment of cancer with drugs that can destroy cancer cells. These drugs often are called "anticancer" drugs. Normal cells grow and die in a controlled way. When cancer occurs, cells in the body that are not normal keep dividing and forming more cells without control. Anticancer drugs destroy cancer cells by stopping them from growing or multiplying. Healthy cells can also be harmed, especially those that divide quickly. Harm to healthy cells is what causes side effects. These cells usually repair themselves after chemotherapy. Because some drugs work better together than alone, two or more drugs are often given at the same time. This is called combination chemotherapy.
Radiation therapy
Radiation therapy (also called radiotherapy, x-ray therapy, or irradiation) is the use of a certain type of energy (called ionizing radiation) to kill cancer cells and shrink tumors. Radiation therapy injures or destroys cells in the area being treated (the "target tissue") by damaging their genetic material, making it impossible for these cells to continue to grow and divide. Although radiation damages both cancer cells and normal cells, most normal cells can recover from the effects of radiation and function properly. The goal of radiation therapy is to damage as many cancer cells as possible, while limiting harm to nearby healthy tissue.
Radiation therapy may be used to treat almost every type of solid tumor, including cancers of the brain, breast, cervix, larynx, lung, pancreas, prostate, skin, spine, stomach, uterus, or soft tissue sarcomas. Radiation can also be used to treat leukemia and lymphoma (cancers of the blood-forming cells and lymphatic system, respectively). Radiation dose to each site depends on a number of factors, including the type of cancer and whether there are tissues and organs nearby that may be damaged by radiation.
Clinical trials
Clinical trials, also called experimental cancer treatment or research studies, test new treatments in people with cancer. The goal of this research is to find better ways to treat cancer and help cancer patients. Clinical trials test many types of treatment such as new drugs, new approaches to surgery or radiation therapy, new combinations of treatments, or new methods such as gene therapy.
A clinical trial is one of the final stages of a long and careful cancer research process. The search for new treatments begins in the laboratory, where scientists first develop and test new ideas. If an approach seems promising, the next step may be testing a treatment in animals to see how it affects cancer in a living being and whether it has harmful effects. Of course, treatments that work well in the lab or in animals do not always work well in people. Studies are done with cancer patients to find out whether promising treatments are safe and effective.
The patients who take part may be helped personally by the treatment(s) they receive. They get up-to-date care from cancer experts, and they receive either a new treatment being tested or the best available standard treatment for their cancer. Of course, there is no guarantee that a new treatment being tested or a standard treatment will produce good results. New treatments also may have unknown risks. But if a new treatment proves effective or more effective than standard treatment, study patients who receive it may be among the first to benefit. Some patients receive only standard treatment and benefit from it.
Complementary and alternative medicine
Complementary and alternative medicine (CAM) is a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine. It is important that the same scientific evaluation that is used to assess conventional approaches can be used to evaluate CAM therapies. In the United States, current trials are underway to test the following:
- acupuncture to reduce the symptoms of advanced colorectal cancer,
- combination chemotherapy plus radiation therapy with or without shark cartilage in the treatment of patients who have non-small cell lung cancer that cannot be removed by surgery,
- hyperbaric oxygen therapy with laryngectomy patients (people who have had an operation to remove all or part of the larynx (voice box)),
- massage therapy for cancer-related fatigue,
- chemotherapy compared with pancreatic enzyme therapy plus specialized diet for the treatment of pancreatic cancer, and
- mistletoe extract and chemotherapy for the treatment of solid tumors.
-
Causes and pathophysiology
Cancer is caused by the accumulation of multiple mutations in the DNA of a cell. Once a single cell becomes cancerous it, over time, expands into a large tumor. Mutations can be caused by many different mechanisms, not all are known. In addition, not all mutations lead to cancer. Hence, the cause for a specific case of cancer cannot usually be identified in the way that the cause of chicken pox can be attributed to transmission of Varicella-zoster virus. Instead, different factors impart a probabilistic risk to developing cancer.
Morphology
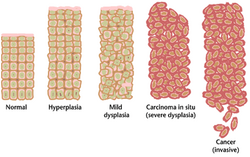 Tissue can be organized in a continous spectrum from normal to cancer.
Tissue can be organized in a continous spectrum from normal to cancer.Cancer tissue has a distinctive appearance under the microscope. Among the distinguishing traits are a large number of dividing cells, variation in nuclear size and shape, variation in cell size and shape, loss of specialized cell features, loss of normal tissue organization, and a poorly defined tumor boundary.
Instead of finding a benign or malignant tumor, microscopic examination of a biopsy specimen will sometimes detect a condition called "hyperplasia". Hyperplasia refers to tissue growth based on an excessive rate of cell division, leading to a larger than usual number of cells. Nonetheless, cell structure and the orderly arrangement of cells within the tissue remain normal, and the process of hyperplasia is potentially reversible. Hyperplasia can be a normal tissue response to an irritating stimulus. For example, a callus that may form on your hand when you first learn to swing a tennis racket or a golf club is produced by hyperplasia.
In addition to hyperplasia, microscopic examination of a biopsy specimen can detect another type of noncancerous condition called "dysplasia." Dysplasia is an abnormal type of excessive cell proliferation characterized by loss of normal tissue arrangement and cell structure. Often such cells revert back to normal behavior, but occasionally, they gradually become malignant. Because of their potential for becoming malignant, areas of dysplasia should be closely monitored by a health professional. Sometimes they need treatment.
The most severe cases of dysplasia are sometimes referred to as "carcinoma in situ." In Latin, the term "in situ" means "in place", so carcinoma in situ refers to an uncontrolled growth of cells that remains in the original location. However, carcinoma in situ may develop into an invasive, metastatic malignancy and, therefore, is usually removed surgically, if possible.
[edit]Molecular biology
Carcinogenesis (meaning literally, the creation of cancer) is the process of derangement of the rate of cell division.
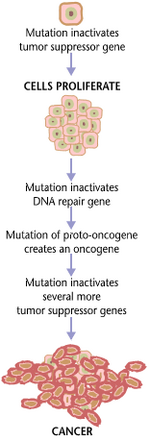 Cancers are caused by a series of mutations. Each mutation alters the behavior of the cell somewhat.
Cancers are caused by a series of mutations. Each mutation alters the behavior of the cell somewhat.Cancer is, ultimately, a disease of genes. Typically, a series of several mutations is required before a cell becomes a cancer cell. The process involves both oncogenes and tumor suppressor genes. Oncogenes promote cancer when "switched on" by a mutation, whereas tumor suppressor genes prevent cancer unless "switched off" by a mutation. Chromosomal translocation, such as the Philadelphia chromosome, is a special type of mutation and may involve oncogenes or tumor suppressor genes. In general, mutations in both types of genes are necessary, as a mutation limited to an oncogene would be suppressed by normal mitosis control.
Mutations can have various causes. Particular causes have been linked to specific types of cancer. Tobacco smoking is associated with lung cancer. Prolonged exposure to radiation, particularly ultraviolet radiation from the sun, leads to melanoma and other skin malignancies. Breathing asbestos fibers is associated with mesothelioma. In more general terms, chemicals called carcinogens and free radicals are known to cause mutations. Chronic inflammation may induce malignancy, as neutrophil granulocytes secrete free radicals.
Mutations can also be inherited. Inheriting certain mutations in the BRCA1 gene renders a woman much more likely to develop breast cancer.
Some types of viruses can cause mutations. They play a role in about 15% of all cancers. Tumor viruses, such as some retroviruses, herpesviruses and papillomaviruses, usually carry some oncogene or tumor suppressor inactivating gene in their genome.
It is impossible to tell the initial cause for any specific cancer. However, with molecular biology, it is now possible to characterize the mutations within a tumor, and to a certain extent predict its behavior. For example, about half of the tumors are deficient in the tumor suppressor gene p53, also known as "the guardian of the genome". This mutation is associated with poor prognosis, since those tumor cells are less likely to go into apoptosis (programmed cell death) when damaged by therapy. There are more mutations that make a tumor more malignant. Telomerase mutations enable a tumor cell to divide indefinitely. Other mutations enable the tumor to grow new blood vessels to feed it, or to detach from the surrounding tissue, spreading to other parts of the body.
Malignant tumors cells, such as in carcinoma, sarcoma, lymphoma or leukemia, have distinct properties:
- evading apoptosis
- unlimited growth potential (immortalitization)
- self-sufficiency of growth factors
- insensitivity to anti-growth factors
- increased cell division rate
- altered ability to differentiate
- no ability for contact inhibition
- ability to invade neighbouring tissues
- ability to build metastases at distant sites
- ability to promote blood vessel growth (angiogenesis)
A cell that degenerates into a tumor cell does usually not acquire all these properties at once, but its descendant cells are selected to build them. This process is called clonal evolution. A first step in the development of a tumor cell is usually a small change in the DNA, often a point mutation, which leads, among other things, to a genetic instability of the cell. The instability increases to a point where the cell loses whole chromosomes, or has double ones. Also, the DNA methylation pattern of the cell changes, activating and deactivating genes more or less at random. Cells that divide at a high rate, such as epithelials, show a higher risk of becoming tumor cells than those which divide less, for example neurons.
In cellular model systems, cells are exposed to carcinogenic influences (chemicals, radiation). In these systems, the first signs of a cell developing into a tumor cell are:
- Immortality. The usual number of cell divisions for a mammalian cell is 50-60 (cell senescence), then it ceases to divide. Tumor cells keep dividing forever.
- Altered morphology.
- Building of cellular clusters (foci).
- Loss of contact inhibition.
- Low or no need for growth factors.
Items 2-4 (above) can sometimes be traced to mutations in genes that result in a disruption of cell adhesion. Some cell adhesion proteins are tumor suppressor genes.
Heredity
Most forms of cancer are sporadic, and have no basis in heredity. There are, however, a number of recognised syndromes of cancer with a hereditary component. Examples are:
- breast cancer and ovarian cancer in female carriers of BRCA1
- tumors of various endocrine organs in multiple endocrine neoplasia (MEN types 1, 2a, 2b)
- Li-Fraumeni syndrome (various tumors such as osteosarcoma, breast cancer, soft-tissue sarcoma, brain tumors) due to mutations of p53
- Turcot syndrome (brain tumors and colonic polyposis)
- Familial adenomatous polyposis an inherited mutation of the APC gene that leads to early onset of colon carcinoma.
Environment and diet
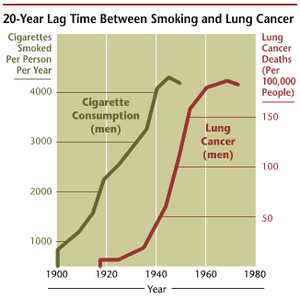 The incidence of lung cancer is highly correlated with smoking.
The incidence of lung cancer is highly correlated with smoking.The most consistent finding, over decades of research, is the strong association between tobacco use and cancers of many sites. Hundreds of epidemiologic studies have confirmed this association. Further support comes from the fact that lung cancer death rates in the United States have mirrored smoking patterns, with increases in smoking followed by dramatic increases in lung cancer death rates and, more recently, decreases in smoking followed by decreases in lung cancer death rates in men.
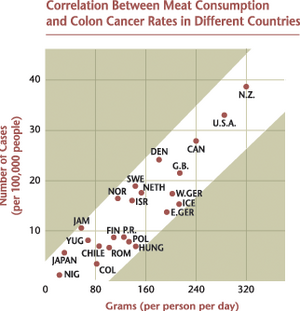 Diet is correlated with the incidence of colorectal cancers.
Diet is correlated with the incidence of colorectal cancers.Prevention
Prevention is defined as the reduction of cancer mortality via reduction in the incidence of cancer. This can be accomplished by avoiding a carcinogen or altering its metabolism; pursuing lifestyle or dietary practices that modify cancer-causing factors or genetic predispositions; and/or medical intervention (chemoprevention) to successfully treat preneoplastic lesions.
Much of the promise for cancer prevention comes from observational epidemiologic studies that show associations between modifiable life style factors or environmental exposures and specific cancers. Evidence is now emerging from randomized controlled trials designed to test whether interventions suggested by the epidemiologic studies, as well as leads based on laboratory research, result in reduced cancer incidence and mortality.
Additional examples of modifiable cancer risk factors include alcohol consumption (associated with increased risk of oral, esophageal, breast, and other cancers), physical inactivity (associated with increased risk of colon, breast, and possibly other cancers), and being overweight (associated with colon, breast, endometrial, and possibly other cancers). Based on epidemiologic evidence, it is now thought that avoiding excessive alcohol consumption, being physically active, and maintaining recommended body weight, may all contribute to reductions in risk of certain cancers; however, compared with tobacco exposure, the magnitude of effect is modest or small and the strength of evidence is often weaker. Other lifestyle and environmental factors known to affect cancer risk (either beneficially or detrimentally) include certain sexual and reproductive practices, the use of exogenous estrogens, exposure to ionizing radiation and ultraviolet radiation, certain occupational and chemical exposures, and infectious agents.
Food and nutrient intake have been examined in relation to many types of cancer. Fruit and vegetable consumption have generally been found in epidemiologic studies to be associated with reduced risk for a number of different cancers; however, it is not currently known which specific components of fruits and vegetables are responsible for the observed associations or if healthy diets are simply associated with other beneficial interventions, e.g., exercise. Contrary to expectation, randomized trials found no benefit of beta-carotene supplementation in reducing lung cancer incidence and mortality; risk of lung cancer was statistically significantly increased in smokers in the beta-carotene arms of 2 of the trials. Similarly, randomized controlled trials have found no reduction in risk of subsequent adenomatous polyps of the colon in individuals who have had polyps resected taking dietary fiber supplements compared with those receiving much lower amounts of supplemental wheat bran fiber. On the other hand, there is evidence from at least 1 randomized controlled trial that calcium supplementation does modestly reduce risk of adenoma recurrence. The "chemoprevention database"[1] (http://www.inra.fr/reseau-nacre/sci-memb/corpet/indexan.html) gives results of all published randomized controlled trials. Consumption of red meat and inadequate folic acid intake have also been associated with increased risk of colon cancer. A large randomized trial is currently underway to investigate whether men taking daily selenium or vitamin E or both experience a reduced incidence of prostate cancer in comparison to men taking placebo pills.
Daily use of tamoxifen, a selective estrogen receptor modulator, for up to 5 years, has been demonstrated to reduce the risk of developing breast cancer in high-risk women by about 50%. Cis-retinoic acid also has been shown to reduce risk of second primary tumors among patients with primary cancers of the head and neck. Finasteride, an alpha-reductase inhibitor, has been shown to lower the risk of prostate cancer. Other examples of drugs that show promise for chemoprevention include COX-2 inhibitors (which inhibit the cyclooxygenase enzymes involved in the synthesis of proinflammatory prostaglandins).
Considerable research effort is now devoted to the development of vaccines to prevent infection by oncogenic agents, and to potential venues for gene therapy for individuals with genetic mutations or polymorphisms that put them at high risk of cancer. Meanwhile, genetic testing for high-risk individuals, with enhanced surveillance or prophylactic surgery for those who test positive, is already available for certain types of cancer, including breast and colon cancers.
Coping with cancer
There are many local organizations that offer a variety of practical and support services to people with cancer. Support can take the form of support groups, counseling, advice, financial assistance, transportation to and from treatment, or information about cancer. Neighborhood organizations, local health care providers, or area hospitals are a good place to start looking.
While some people are reluctant to seek counseling, studies show that having someone to talk to reduces stress and helps people both mentally and physically. Counseling can also provide emotional support to cancer patients and help them better understand their illness. Different types of counseling include individual, group, family, self-help (sometimes called peer counseling), bereavement, patient-to-patient, and sexuality.
Many governmental and charitable organizations have been established to help patients cope with cancer. These organizations often are involved in cancer prevention, cancer treatment, and cancer research. Examples include: American Cancer Society, BC Cancer Agency, Cancer Research UK, Canadian Cancer Society, International Agency for Research on Cancer, National Cancer Institute (US), and Yorkshire Cancer Research.
Social impact
Cancer has a reputation for being a deadly disease. While this certainly applies to certain particular types, this is otherwise a generalization. Some types of cancer have a prognosis that is substantially better than nonmalignant diseases such as heart failure and stroke.
Progessive and disseminated malignant disease has a substantial impact a cancer patient's quality of life, and many cancer treatments (such as chemotherapy) may have severe side-effects. In the advanced stages of cancer, many patients need extensive care, affecting family members and friends. Palliative care solutions may include permanent or "respite" hospice nursing.
Cancer research
Cancer research is the intense scientific effort to understand disease processes and discover possible therapies. While understanding of cancer has increased exponentially since the last decades of the 20th century, radically new therapies are only discovered and introduced gradually. Inhibitors of tyrosine kinases (imatinib and gefitinib) in the late 1990 were considered a major breakthrough, as they interfere with cancer processes on a molecular level (which chemotherapy does not).
See also
- experimental cancer treatment
- list of cancer patients
- list of oncology-related terms
- oncology
- palliative care
- terminal illness
- United Devices Cancer Research Project
References
- How To Find Resources in Your Own Community If You Have Cancer (http://cis.nci.nih.gov/fact/8_9.htm), National Cancer Institute Fact Sheet.
- Taking Part in Clinical Trials: What Cancer Patients Need To Know (http://cancer.gov/clinicaltrials/resources/taking-part-treatment-trials), National Cancer Institute Fact Sheet.
- Complementary and Alternative Medicine (http://cis.nci.nih.gov/fact/9_14.htm), National Cancer Institute Fact Sheet.
- The Prostate-Specific Antigen (PSA) Test: Questions and Answers (http://cis.nci.nih.gov/fact/5_29.htm), National Cancer Institute Fact Sheet.
- Cancer Prevention Overview (PDQ®) (http://www.nci.nih.gov/cancertopics/pdq/prevention/overview), National Cancer Institute.
- Ries LAG, Smith MA, Gurney JG, Linet M, Tamra T, Young JL, Bunin GR (eds). Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975-1995, National Cancer Institute, SEER Program. NIH Pub. No. 99-4649. Bethesda, MD, 1999. Chapter XII Cancer among infants (http://seer.cancer.gov/publications/childhood/infant.pdf), James G. Gurney, Malcolm A. Smith, and Julie A. Rosa.
- Radiation Therapy for Cancer: Questions and Answers (http://cis.nci.nih.gov/fact/7_1.htm), National Cancer Institute Fact Sheet.
- Chemotherapy and You: A Guide to Self-Help During Cancer Treatment (http://www.cancer.gov/PDF/b21d0a74-b477-41ec-bdc0-a60bbe527786/chemoandyou.pdf), National Cancer Institute. (NIH Publication No. 03-1136)